18yr old male with difficulty in walking since 1 month
I've been given this case to solve in an attempt to understand the topic of 'Patient clinical data analysis' to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Patient complaint: difficulty in walking since 1 month,
Under evaluation:
distal and proximal muscle weakness and wasting of muscles present ,no sensory and anatomical involvement, hypotonia and decreased power in lower limbs and absent reflexes, no fasiculations
ANATOMICAL location:
Peripheral neuropathy
Axonal: chronic,distal to proximal, reflexes not affected,sensory more involved than motor, wasting minimal ,calf tenderness
Demylinating: acute diffuse proximal and distal, reflexes are lost,motor more involved than sensory,wasting not seen, ncv decreased
Anterior horn cell: wasting present fasiculations present distal affected more no autonomic and sensory
The patient finding are more consistent with axonal periferal NEUROPATHY
PATHOGENESIS
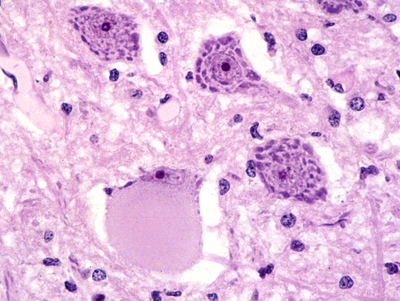
Changes also occur in the neuronal body. The RER disaggregates and the neuronal body balloons. The cytoplasm becomes smooth and the nucleus is displaced toward the periphery of the cell. This process is called central chromatolysis and reflects activation of protein synthesis in order to regenerate the axon.
distal axonopathy, degeneration of axon and myelin develops first in the most distal parts of the axon and, if the abnormality persists, the axon "dies back". This causes a characteristic distal ("stocking-glove") sensory loss and weakness. Neurofilaments and organelles accumulate in the degenerating axon (probably due to stagnation of axoplasmic flow). Eventually the axon becomes atrophic and breaks down. Severe distal axonopathy resembles Wallerian degeneration. At an advanced stage, there is loss of myelinated axons. Many clinically important neuropathies caused by drugs and industrial poisons such as pesticides, acrylamide, organic phosphates, and industrial solvents are characterized by distal NEUROPATHY
Pharmacology: 1)T.B COMPLEX OD
Differential diagnosis:
For peripheral neuropathy
Genetic disorder like charcot Marie tooth disease
Drugs causing peripheral neuropathy are not seen
Like amiadarone,anti retrovirals
Toxins like arsenic and lead are not seen
Vitamin deficiency may be possible
Gillian Barre is not possible because nerve conduction studies are normal

{kind=link}
Comments
Post a Comment